A Patient's Guide to Intraoperative Monitoring
Introduction
Spine surgery can be unpredictable and potentially dangerous because it can involve areas near nerves and the spinal cord. During spinal surgery, there is a risk that damage to the nervous system can occur. This is especially true when hardware or instrumentation is used and inserted near nerves, or when a curvature of the spine is corrected. It is important for surgeons to be able to have someone experienced to monitor nerve tissue while doing the operation.
The nervous system can be monitored during spine surgery to make it safer. The term commonly used for monitoring the nervous system during surgery is intraoperative monitoring, or intraoperative neurophysiologic monitoring (IOM). Intraoperative monitoring is not only being used for complex spinal surgeries but is widely used for other surgeries too. Some of these include brain surgery, ear surgery, and surgery involving arteries.
This guide will help you understand
- what is intraoperative monitoring
- why is intraoperative monitoring important
- when is intraoperative monitoring used
- what happens during surgery
- what are possible complications
Anatomy
What parts of the spine are involved?
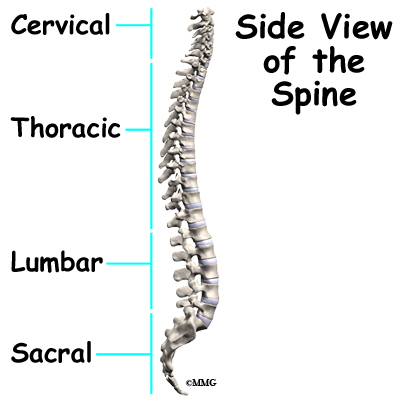
The spine is divided into various parts. The upper portion is the cervical spine, or neck. The middle portion is the thoracic spine, or trunk. The lower portion is the lumbar spine, or low back. There are bony blocks called vertebrae that make up the spine. They are stacked on top of one another. There are discs that separate the vertebrae and provide cushion. The spinal cord is protected by the bony spine. It lies in a hollowed area, or arch made by the bony spine. This is called the spinal canal.
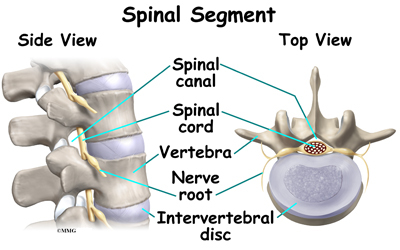
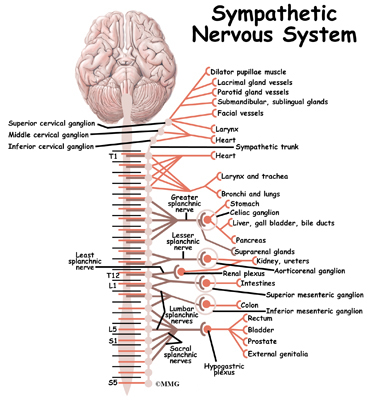
Projecting from the spinal cord are nerves that travel to limbs, the trunk, and internal organs. The spinal cord is similar to a tree trunk. The nerves are like branches. The portion of the nerve as it branches off of the spinal cord is called the nerve root. The spinal cord sends and receives messages to and from the body and the brain. The nerves that branch off of the spinal cord go to various body parts to provide sensation and motor function or movement.
Nerve tissue is delicate and can be damaged relatively easily. When damage is done to the spinal cord or nerve, it may cause sensory and/or motor changes in the affected body part. The damage may be permanent.
What is intraoperative monitoring?
Intraoperative neurophysiological monitoring (IOM) uses equipment to evaluate the function of the spinal cord and nerves during spine surgery. Its role is to provide the surgeon with immediate feedback and warning before permanent nerve injury has occurred. This has been shown to increase safety and improve outcomes in complex spine surgery.
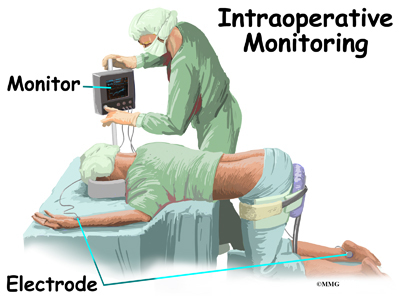
Intraoperative neurophysiological monitoring (IOM) began with the use of somatosensory evoked potentials (SSEPs). This measures the conduction of sensation above and below the area of surgery. During spinal surgery, electrodes are placed on limbs that could be affected by the surgery. Electrodes are also placed on the surface of the skull over the area of the brain where the impulse from the limb is received. A machine is used to monitor the electrical activity in the brain just like an electroencephalogram (EEG). The electrical activity is recorded as waves. When the limb is stimulated with an electrical current by the surgeon or technician, there should be a response in the brain. This checks the function of the sensory portion of the nerves and spinal cord.
Somatosensory evoked potentials (SSEPs) are the most widely used intraoperative neurophysiological monitoring during surgery. However, SSEP monitoring may not detect injuries to individual nerve roots.
In the 1980s surgeons began using electromyography (EMG) to monitor the motor portion of the nerves during spinal surgery. It is becoming more commonly used. During surgery, while the patient is asleep, needle electrodes are placed in the muscle groups that correspond to the area where the surgeon will be working. Electrical activity from the muscle can be monitored by a machine. The activity is recorded as waves, similar to the SSEP monitor. It is also similar to the waves that are recorded from the heart muscle during an electrocardiogram (ECG). Baseline recordings are taken before the surgery begins. Recordings are then repeated throughout the procedure. A significant change in the wave alerts the surgeon or technician that the nerve in the area could be damaged. The surgeon can then take action to prevent permanent damage.
EMG seems to be more accurate in identifying potential neurological damage than other methods of monitoring that have been used. However, it is not useful when muscle paralyzing agents are used for anesthesia. It is also not useful if a nerve root has been cut completely.
Studies show that the use of both SSEPs and EMG monitoring during spinal surgery is most ideal but not always available.
Other monitoring available includes rectal and urinary sphincter electromyography, motor-evoked potentials (MEPs), transcranial electrical stimulation (TES), brainstem auditory evoked potential (BAEP), dermatomal evoked potentials (DEP), facial nerve monitoring, and spinal cord mapping.
Why is intraoperative monitoring important?
Spine surgery can be unpredictable and dangerous because it can involve areas near nerves and the spinal cord. During spinal surgery there is a risk that damage to the nervous system can occur. Intraoperative neurophysiological monitoring allows the surgeon to know, during the surgery, if/when nerve tissue is being injured or is at risk for being injured. The problem can be corrected immediately. Intraoperative neurophysiological monitoring (IOM) allows assessment of nerve tissue function while the surgery is taking place. Many complications involving the nervous system can be avoided with careful monitoring during surgery. This makes spine surgery safer. It is also proven to improve the outcomes of spinal surgery. It is being used more commonly, especially during complicated spinal surgery.
Spine surgery often involves the use of instrumentation (hardware). This hardware may include screws, rods, plates, and cages. The complication rate from instrumentation with lumbar spine fusion varies from one to 33 per cent. Possible complications from placement of hardware include damage to the spinal cord and nerve roots. Up to 10 per cent of the time, pain and sensory changes in the portion of the limb affected can result. This is called radiculopathy. One per cent of the time, motor change or weakness in the portion of the limb affected at that surgical level can occur. This is called myelopathy. Neither of these outcomes is desirable after spine surgery.
Surgeons have relied on imaging, most usually X-rays and computed tomography (CT) scans to check the placement of hardware during surgery. However, there are times when these do not show improperly placed hardware, fracture of spinal bone, or damage to nerve tissue.
Intraoperative neurophysiological monitoring (IOM) is more effective in sensing neurological damage, and misplacement of hardware. In fact, some studies show that it is one-third more effective than imaging with X-ray or CT scan.
Until intraoperative neurophysiological monitoring, surgeons commonly relied on the wake up test and the clonus test to evaluate nerve function during surgery. However, these are more difficult to repeat during the surgery, can lengthen the time of surgery, and do not fully evaluate nerve function. The wake up test involves allowing the patient to wake up from the anesthesia. The patient is then asked to move body parts that may be affected by the surgery. The clonus test involves the surgeon quickly jerking the foot towards the shin to see if the stretch reflex still works. This assesses the function of the spinal cord.
Intraoperative neurophysiological monitoring (IOM) is quick, painless, easy, and inexpensive. Recordings can be taken several times during surgery or even throughout the entire procedure. It does not cause harm to the patient. It also provides real-time feedback to the surgeon. It is safe and effective for reducing nerve tissue damage during surgery.
When is intraoperative monitoring used for spinal surgery?
Some spine surgeons may prefer to use intraoperative monitoring during most (if not all) of their surgeries. Others prefer to use it during complex surgeries. It is commonly used for the following spinal surgeries:
- All spinal cord cases
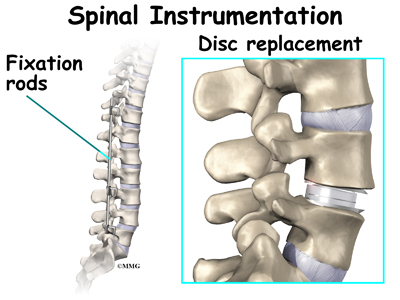
- Spinal instrumentation with hardware
- Scoliosis
- Discectomy with a neurological deficit
- Decompression with a neurological deficit
- Total disc replacement
- Pain stimulator placement
- Corpectomy
- Vertebrectomy
- Odontoid/Dens fractures
What happens during surgery?
After you are put to sleep by the anesthesiologist, small wire electrodes are placed in the muscles of your lower leg for lumbar surgery. They may be placed in the arms for neck surgery. For EMG monitoring, the electrodes are placed in specific muscles that correspond with a specific level in the spinal cord.
Technically, EMG monitoring is relatively easy, and the setup takes practically no additional time during positioning for the surgical procedure.
Intraoperative monitoring is technically done by a technician who is in the operating room during the entire procedure. A neurophysiologist may be involved in interpreting the recordings generally at a remote location where they observe the same data as seen by the technologist. This real-time interpretation by an experienced neurophysiologist is the standard of care in many regions in the United States.
If the spinal cord or nerve roots are damaged while drilling into bone, placing hardware in the spine, or decompressing the spine, the SSEP or EMG signal will change. This alerts the technician who can then alert the surgeon. Some monitoring units are equipped with a loudspeaker that allows immediate audio feedback. The surgeon can make a change at that time to avoid damage to nerve tissue.
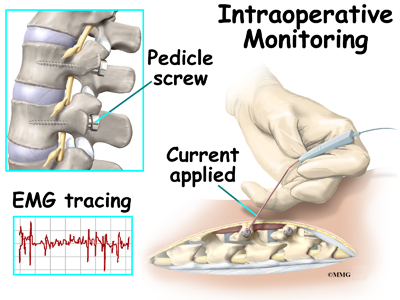
When pedicle screws are used, the surgeon may use a handheld probe that can give an electrical stimulation to the pedicle screw once it has been placed. If the screw is where it is supposed to be, it will take a certain amount of current to cause a muscle contraction and wave on the monitor. If it is misplaced, it will take less. This is called an evoked EMG.
The surgeon can then re-evaluate the placement of the screw in order to avoid harm to the nerve root or spinal cord.
SSEPs and EMG recordings can be taken several times during the surgery if necessary without causing harm to the patient.
What are possible complications of intraoperative monitoring?
There really are none. The surgery need not be interrupted unnecessarily during surgery when neurophysiological monitoring is used. This is safer for the patient. Because the skin is penetrated with needle electrodes, there is a small risk for infection. This is minimal as the skin is disinfected before the needles are placed. The needles are sterile. They are thrown away after a single use. Mild soreness may be experienced where the needles were inserted.
Intraoperative monitoring is usually not costly. It is well worth it to avoid neurological complications during spinal surgery when possible.
|





